Melanoma
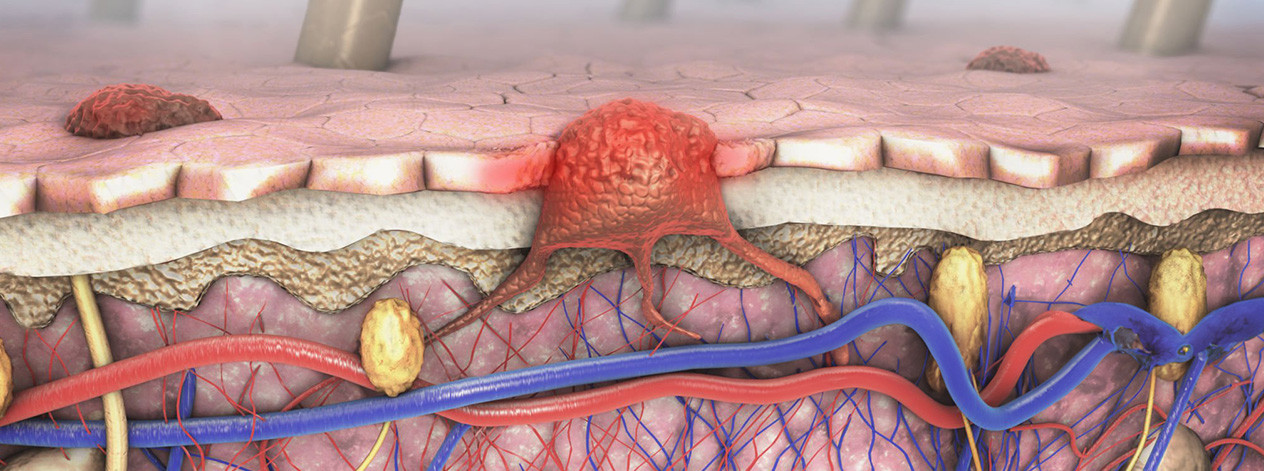
Malignant melanoma is predominantly a disease of the skin, but may in rare instances occur at other sites, including the mucous membranes (vulva, vagina, lip, throat, esophagus and perianal region), as well as in the eye (uvea and retina). Melanoma arises from melanocytes, which are cells located in the upper layer of the skin that are responsible for producing pigment (skin color). Most melanomas are dark in color (black/brown) because they contain pigment; however, some melanomas do not contain pigment (amelanotic malignant melanoma) and are difficult to diagnose.
Since the majority of patients enrolled in clinical trials have skin (cutaneous) melanoma, this treatment overview will focus on that type of melanoma. It is important to realize that the treatment principles derived from clinical trials involving patients with skin melanoma are applicable to melanomas of the vulva, vagina, male genitalia or anorectal areas but, in general, melanomas in these sites have a worse prognosis than skin melanomas. Melanoma occurs predominantly in adults, who comprise most of the 54,000 new cases per year in the U.S. The incidence of melanoma of the skin appears to be on a steady rise throughout the world due to increased ultraviolet exposure from the sun and possibly tanning beds. In the United States, researchers have estimated that there is a 2-3% increase per year in the incidence of cutaneous melanoma. Approximately 7,000 individuals in the U.S. die of malignant melanoma every year.
In order to diagnose malignant melanoma, a physician will remove the primary cancer and a pathologist will examine the tumor under the microscope. Once melanoma is diagnosed, there are two critical factors that need to be determined: the thickness of the tumor and whether or not the cancer has spread (metastasized) to other parts of the body. These factors are part of the staging procedures for melanoma. It is important to determine the stage of disease in order to determine treatment options and outcomes.
Thickness: The most important feature of the tumor is the thickness, which is measured in millimeters. Melanoma is divided into 3 groups based on thickness: (a) thin melanomas (< 1 mm thickness), (b) intermediate melanomas (1 to 4 mm in thickness), and (c) thick melanomas (> 4 mm). The thickness of the tumor is important because it will have an impact on whether the tumor has spread, which is the other critical factor used to determine the stage of disease. The thicker a melanoma is, the more likely it is to have spread to lymph nodes at the time of diagnosis.
Spread: In general, when melanoma spreads, it spreads to lymph nodes in the region of the tumor first. Lymph nodes are small, bean-shaped structures that are part of the immune system. They are found throughout the body and are interconnected by lymph channels. Melanoma tends to spread through lymph channels that drain into lymph nodes in the local area of the primary skin melanoma. Once a pathologist has determined the thickness of the tumor, the next step in pathological staging may involve surgical removal and examination of the local lymph nodes to determine if apparently normal lymph nodes contain melanoma cells.
Over the past decade, sentinel lymph node (SLN) biopsy techniques have improved the ability to detect small amounts of tumor in lymph nodes. SLN biopsy is a technique that relies on intra-operative lymphatic mapping. During a SLN biopsy, a physician injects a tracer (radioactive isotope and/or blue dye) into the area of the primary tumor. The tracer, which is taken up by the lymph system, identifies the so-called “sentinel lymph node” (SLN), which is the first lymph node that could be potentially involved with melanoma. Lymphatic mapping can be performed prior to surgery to aid the physician in determining which lymph node group is the primary drainage basin for any particular area of skin and it can also be used on the day of surgery to identify which lymph node is the first node (sentinel lymph node).
During a SLN biopsy, the physician removes the SLN through a small incision and then a pathologist examines the SLN under the microscope to detect whether or not there is any evidence of melanoma cells. Patients who have a positive sentinel node (tumor identified) are counseled to undergo removal of all the lymph nodes in the region, while patients who have a negative sentinel node do not undergo further surgery. Although there is an intense effort to develop blood tests for detecting metastatic disease, none have proven completely reliable. There is evidence that surgical removal of involved lymph nodes may improve survival. This may especially be true when only one lymph node is involved with melanoma. Ideally, if there is no melanoma involvement in the lymph nodes, the removal of lymph nodes should be avoided. It is important to know about the presence of local lymph nodes involved with spread of melanoma, as this is one of the criteria frequently used to identify patients at high risk for development of recurrent disease and is also an entry criteria for clinical trials evaluating the role of additional therapy.
Melanoma can spread by local extension (through the lymph system, as described above) and/or by the blood to distant sites. Satellite lesions can also occur in the skin adjacent but separate from the primary melanoma. These are sometimes called in-transit metastases, implying that secondary melanomas have grown in the skin on their way to spreading to local lymph nodes. Any organ can be involved by metastases from malignant melanoma, but the lungs and liver are the most common sites.
In 3-5% of patients, melanoma is present in lymph nodes or other organs without an identifiable primary site and these patients are said to have “melanoma of unknown origin.” In such cases, it is believed that the primary melanoma underwent spontaneous regression, while the metastasis remained. Patients with unknown primary in the lymph nodes or in distant sites have stage III or IV disease and are treated as outlined for malignant melanomas of these stages.

Treatment Outcomes: Most patients with disease localized to the skin can be cured with surgery. The majority of patients with spread of melanoma to local lymph nodes cannot be cured with current therapies. The average survival of patients with melanoma that has spread outside the local area is only 7.5 months, with only 5-10% of patients surviving beyond 5 years. Thus, there is a great interest in improving early diagnosis, which is the most effective way of improving the cure rate for patients with melanoma. There is generally a survival advantage for females over males for all stages of disease. In Scotland, the melanoma-free survival for men is reported to be 69% at 5 years, compared to 82% for women.
Melanoma is one of the few cancers that has shown regression without treatment. Spontaneous partial regression can be common, but complete and permanent regression is rare, with only 33 cases being documented in the world’s literature. It has been suggested that spontaneous regressions occur because the patient’s immune system rejects the cancer. This observation has caused physicians to try treatments with interferons, interleukins, vaccines and other treatments that stimulate the immune system to react against the malignant melanoma.
Prognosis: For disease confined to the site of origin, the greater the thickness or depth of local invasion of the melanoma, the higher the chance of lymph node metastases and the worse the prognosis. Following surgery, the highest risk of recurrence is within the first two years, but late relapses are not uncommon.
Staging System: The staging system for melanoma has recently been revised, but continues to be based on primary tumor thickness, ulceration of the primary tumor, lymph node involvement, and distant metastasis. Historically, the staging system for primary melanoma was based on the Clark’s level and Breslow thickness. A common mistake with a new diagnosis has been to confuse Clark’s level with stage. Unlike stage, the Clark’s level describes a primary melanoma tumor microscopically, dividing the skin into 5 levels and assigning the melanoma to a different level based on how deep the melanoma penetrated.
- Clark’s Level I: Melanomas confined to the outermost layer of the skin, the epidermis. Also called “melanoma in-situ.”
- Clark’s Level II: Penetration by melanomas into the second layer of the skin, the dermis.
- Clark’s Levels III-IV: Melanomas invade deeper through the dermis, but are still contained completely within the skin.
- Clark’s Level V: Penetration of melanoma into the fat of the skin beneath the dermis, penetration into the third layer of the skin, the subcutis.
Since the division of skin layers and skin thickness is variable, the Clark’s level is somewhat subjective according to the pathologist making the reading. Due to its subjectivity and variability, the Clark’s Level is a less significant prognostic factor in the new staging system. However, the Breslow thickness continues to be an important measurement since it is more exact, more reproducible, and less subjective. The Breslow thickness is measured in millimeters and defines the vertical thickness (how far tumor extends into the skin) of a primary melanoma.
The Tumor-Node-Metastasis (TNM) classification system may also be encountered in melanoma staging. The TNM classification is used by pathologists to stage melanoma by describing tumor thickness, nodal involvement and presence of metastasis.
Recent studies indicate that ulceration (microscopic absence of continuous epidermis in tissue overlying the melanoma) of the primary tumor, the number of lymph nodes involved, sites of distant metastases and elevation in levels of blood enzyme called lactate dehydrogenase (LDH) are the most valuable prognostic factors for melanoma. A revised staging system by the American Joint Committee on Cancer (AJCC) took effect nationwide in January 2003.
The following is a simplified staging system useful for determining treatment and estimating outcomes. This staging system implies that the status of local lymph nodes is known from examination under the microscope. If direct surgical examination is not done, some patients staged as clinical stage II will in fact have stage III disease with lymph node involvement. In order to learn more about the most recent information available concerning the treatment of melanoma cancer, click on the appropriate stage.
Melanoma in Situ: Malignant melanoma cells are found only in the outer layer of skin cells (epidermis) and have not invaded to deeper layers.
Stage I: Malignant melanoma is found in the outer layer of the skin (epidermis) and/or the upper part of the inner layer of skin (dermis), but has not spread to lymph nodes. The melanoma is < 1 mm with or without ulceration or 1-2 mm without ulceration. Stage I melanoma is further divided into stage IA and IB.
- Stage IA: The malignant melanoma is not more than 1 millimeter (less than 1/16 of an inch) thick, with no ulceration. The tumor is in the epidermis and upper layer of the dermis.
- Stage IB: The malignant melanoma is either not more than 1 millimeter thick, with ulceration, and may have spread into the dermis or the tissues below the skin; or 1 to 2 millimeters (more than 1/16 inch) thick, with no ulceration.
Stage II: The malignant melanoma is 1 to 2 millimeters with ulceration or > 2 mm with or without ulceration. Malignant melanoma has spread to the lower part of the inner layer of skin (dermis), but has not spread into the tissue below the dermis or into nearby lymph nodes. Stage II melanoma is further divided into stage IIA, IIB and IIC.
- Stage IIA: The malignant melanoma is either 1 to 2 millimeters thick, with ulceration; or 2 to 4 millimeters (a little more than 1/8 of an inch) thick, with no ulceration.
- Stage IIB: The malignant melanoma is either 2 to 4 millimeters thick, with ulceration; or more than 4 millimeters thick, with no ulceration.
- Stage IIC: The malignant melanoma is more than 4 millimeters thick, with ulceration.
Stage III: The malignant melanoma can be any thickness with spread to regional lymph nodes. Stage III melanoma is further divided into stage IIIA, IIIB and IIIC.
- Stage IIIA: The malignant melanoma may have spread to as many as 3 nearby lymph nodes, but can only be seen with a microscope.
- Stage IIIB: The malignant melanoma has either spread to as many as 3 lymph nodes and may not be visible without a microscope; or has satellite tumors (additional tumor growths within 1 inch of the original tumor) and has not spread to lymph nodes.
- Stage IIIC: The malignant melanoma has either spread to as many as 4 or more lymph nodes and can be seen without a microscope; or has lymph nodes that may not be moveable; or has satellite tumors and may have spread to lymph nodes.
Stage IV: The primary malignant melanoma is any size, but has spread to distant lymph nodes and/or distant sites.
Locally Recurrent Melanoma: Malignant melanoma has recurred, but is limited to skin and/or regional lymph nodes.
Recurrent and Refractory Stage IV Melanoma: Patients who have not responded to or progressed after initial systemic therapy (chemotherapy and/or biologic therapy) or have malignant melanoma that has recurred.
Copyright © 2020 Omni Health Media Melanoma Information Center. All Rights Reserved.